
Anorectal Malformation in children – causes, symptoms & treatment in Malaysia
Before we start understanding Anorectal Malformation in Children in Malaysia, let us examine the part of the body affected by ANO-RECTAL Malformation …
ANO- stand for the anus – this is the opening at the bottom end of the large intestine. Stool comes out through here when there is a bowel movement. -RECTAL means the rectum, this is the part of the large intestine just above the anus.

During normal bowel movement, stool passes from the large intestine to the rectum and then through the anus. Muscles in the anal area help to control when you have a bowel movement and nerves in the area help the muscles sense the need for a bowel movement and also contract and relax the muscle of the anus.
There should be individual episodes of bowel opening when the anal musculature relaxes and the bowel muscles contracts and expels the faeces. Till the next episode, they often remain clean.
What is Anorectal Malformation?
Anorectal Malformation (ARM) is a birth abnormality to the bottom end of the intestinal tract where the opening is inadequate or in the wrong position. There are different forms of this anomaly for girls and boys. In some there is an abnormal opening that’s visible where there may be faeces coming out of and in others there are no visible opening at the bottom.

What causes Anorectal Malformation (ARM)?
It is thought that the urinary system and the bowel tract opened into one common opening during the early developing human, during the early part of pregnancy. It then separates to the urinary system in front and the rectum/anus at the back. Failure of this separation process to happen may lead to an abnormality as to where the rectum opens.
Anorectal malformations occur in around 1 in 5,000 babies.
They are slightly more common in males. Most babies with ARM do not have a family history of this. There is however a strong association of ARM with children born with Downs Syndrome.
What are the symptoms of Anorectal Malformation
Common symptoms of ARM are:
Lack of stool
Stool coming from the vagina
Stool in the urine
Urine coming from the anus
Trouble having a bowel movement, or constipation
What are the common forms of Anorectal Malformation?
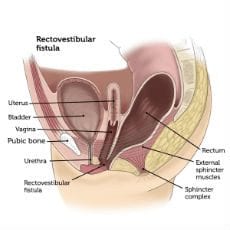
Recto vestibular fistula (girls)
The commonest form of ARM in girls are the recto-vestibular fistula where the rectum opens at the opening of the vagina (not within the vagina). Here we should be able to see the opening of the rectum and faeces can usually be passed.
Recto-Urethral fistula (boys)
In boys the commonest anomaly is a recto urethral fistula, where the rectum is connected to the urethra or urinary tract that is a tube between the bladder to the tip of the penis. Here there are no rectal/anal openings seen and the child will usually need a stoma formed so the baby can feed and defecate.

Perineal fistula (boys and girls)
This is not an obvious form of ARM. However, symptoms that may be apparent early on are: straining to open bowels which happens frequently day or night, abdominal distention, vomiting, poor feeding, constant faecal soiling on the bottom or nappy, breakdown of skin or constipation or obstruction with inability to pass any faeces for a few days in a row. For some, they may not have any symptoms, especially whilst exclusively on breast milk feeds.

just outside the muscle of the anus


Examination & Diagnosis of Anorectal Malformation
Your child’s surgeon will examine your child and assess if there is a problem. Investigations may be necessary to work out a diagnosis.
Your child may also have tests such as:
- Abdominal X-rays. This test images bones (spine and pelvis) and may give likely position of the rectum.
- Abdominal ultrasound. To see soft tissues like the bladder, kidneys and spinal cord.
- Lower GI contrast study. X ray “dye” liquid is placed into the rectum so that they will show up on an X-ray. This is to work out the structure and anatomy of lower bowel.
- Echo cardiogram. A special “ultrasound” of the heart is done to look at its structure and function.
For good bowel functioning, there should be no abnormal kinks or acute bends in the bowel and the rectum should open into the anal canal within the muscle sphincter complex. Hence a smooth passage of faeces and evacuation that can be controlled by the muscle voluntarily. In treating this condition, the rectum will be straightened out if required and should pass through the muscle for control of continence.
Treatment of Anorectal Malformation
Treatment will depend on your child’s symptoms, age, and general health. It will also depend on how severe the condition is. Most babies with an anorectal malformation will need to have surgery to correct the problem.
The type and number of surgeries your child needs will vary depending on the type of problem the child has. These surgeries may include:
Colostomy (stoma)
Some surgeons prefer colostomies, or stoma, for most type of ARM to protect the reconstructive repair from faeces. My preference are for colostomies for ARMs where there are no visible openings. If adequate faeces continues to be expelled without a stoma, this can go on till the definitive surgery is done.
With a colostomy, the large intestine is brought through openings on the tummy. The upper end of the opening of the large intestine (divided into two) lets stool out into a collection bag. The other end lets mucus made by the intestine to pass into the collection bag. This allows your child to grow before the next surgery.

Reconstructive surgery: Attaching the rectum to the anus
This surgery is often done in the first few months of life. The colostomies stay in place for a few months after this surgery. This is so the area can heal without being infected by stool. The rectum and anus are now joined with this procedure.
For most boys, keyhole surgery procedure is best, to avoid painful large cuts at the bottom.
For most girls, the abnormal opening is usually visible so detaching this rectum from an abnormal position and tunnelling it through the muscle to create the new anus can be done via a small incision at the bottom.
A few weeks after surgery, you may be doing anal dilations to prevent the newly created opening from narrowing.

Closing the colostomy
This surgery is done about 2 to 3 months later.
Several days after surgery, your child will start passing stools through the new rectum/anus. At first, stools will be frequent and loose. Diaper rash and skin irritation is a common problem at this stage. However, a few weeks after surgery, the stools frequency is less often and are more solid.
To avoid your child from then becoming constipated, a high-fibre diet and laxatives are usually prescribed.
Recovery & Bowel Management of Anorectal Malformation
The initial task after the surgeries is to prevent constipation. Your doctor will monitor your child regularly to ensure there are no issues with constipation and that your child is developing continence.
Each type of ARM has unique characteristics and it effects each child differently. Whether a child has any problems depends a great deal on the type of ARM the child has and they generally gain bowel control more slowly than children who do not.
The first few years may bring a few challenges but keeping a good communication with your surgeon is key to avoiding any serious issues and when managed well, it avoids any long term psychological issues with your child, related to his or her “bottom”.
Parent Testimonial of Anorectal Malformation Treatment by Dr Nada
“When my son was born in 2013, the doctor found that his anus was different from other children. He needed to do surgery immediately so that he can defecate normally, and this surgery required huge medical fee that I couldn’t afford. I was worried and afraid.
I decided to send my son to Hospital University Malaya. That was the first time I met Prof Nada. He explained in detailed to me that my son needed 3 surgeries.
The first operation was to put the stoma bag to allow him to poo. The second was to create a new anus and the third surgery is to close the stoma. I was worried and fearful every time when my son underwent surgery, but every time when Dr Nada finished the surgery he came out to comfort me.
He is patient , humble and affable doctor. He always has a smile on his face. Dr Nada saved my child and gave him a new life. Now my son is six years old, he has the same bowel movement as a normal child and healthy growth. Dr Nada is kind, professional, and an awesome, remarkable doctor. We are always grateful for everything he had done for my child.”
Ms Lau, mother
Dr Nada in the media with regards to Anorectal Malformation
The case of Lew Cheng Xin and how Da-Ai rallied Malaysian’s to raise RM66,000 for his urgent operation (23-06-2021)



“𝙃𝙞 𝘿𝙧 𝙉𝙖𝙙𝙖 𝙄 𝙟𝙪𝙨𝙩 𝙬𝙖𝙣𝙩 𝙩𝙤 𝙘𝙝𝙚𝙘𝙠 𝙩𝙝𝙚 𝙖𝙪𝙩𝙝𝙚𝙣𝙩𝙞𝙘𝙞𝙩𝙮 𝙤𝙛 𝙇𝙚𝙬 𝘾𝙝𝙚𝙣𝙜 𝙓𝙞𝙣’𝙨 𝙘𝙖𝙨𝙚 𝙖𝙣𝙙 𝙩𝙝𝙚 𝙘𝙧𝙤𝙬𝙙 𝙛𝙪𝙣𝙙𝙞𝙣𝙜 𝙗𝙮 𝘿𝙖 𝘼𝙞 – 𝙏𝙌”
We received a few such messages today from our community in regards to the case of Lew Cheng Xin, and his mother’s (Winnie Lew Qi Voon) appeal for help to cover his urgent surgical costs.
See the full story here and find out how you can help > https://www.facebook.com/DaaiMalaysia.PJ/posts/1186581051857384
The case was shared via DA-AI, a wonderful NGO that aims to help those in need with Social Crowdfunding.
The little boy, Cheng Xin is suffering from 𝗔𝗻𝗼𝗿𝗲𝗰𝘁𝗮𝗹 𝗠𝗮𝗹𝗳𝗼𝗿𝗺𝗮𝘁𝗶𝗼𝗻.
With the letter above, Dr Nada would like to re-assure the community that the case is indeed genuine and he is treating the brave little boy after Winnie brought him to see him.
For Cheng Xin’s sake and that of his mother, Winnie, we hope they get the help they desperately need so that we can focus on his urgent treatment and recovery.
Facebook Post 1: https://www.facebook.com/DrNadaSudhakaran/posts/522404325872459
Facebook Post 2: https://www.facebook.com/DrNadaSudhakaran/posts/525573878888837
Article Published in Easily Sin Chew on 17-12-2020
(click image to link to original post)

















































