
What is Tongue Tie in babies & children – causes, symptoms & treatment in Malaysia
What is Tongue Tie?
Tongue tie or ankyloglossia is a condition present at birth that restricts the tongue’s range of motion.
With tongue tie, an unusually short, thick or tight band of membrane tissue (lingual frenulum) tethers the bottom of the tongue’s tip to the floor of the mouth, so it may interfere with breast-feeding.
The severity varies from a posterior tongue tie ( one which is a thick band, right at the back, at the angle of the tongue and the floor of the mouth), which may not be very obvious, to a severe one to the tip of the tongue with a heart shaped appearance of the tongue tip.

Someone who has tongue tie might have difficulty sticking out his or her tongue. Tongue tie can also affect the way a child eats, speaks and swallows.
Sometimes tongue tie may not cause problems. Some cases may require a simple surgical procedure for correction.
Essentially what is crucial is to ask if the tongue tie is causing functional issues for your child or will it potentially be a problem in the future?

Click HERE for original article.
What Causes Tongue Tie?
As the tongue develops as a fetus, from the back of the mouth forwards, a membrane under the developing tongue follows it forward, this should usually disappear before birth. However in some babies it remains to different degree when born. Some are thin, flimsy and stretchy, others can be thick and short and causes significant limitation of tongue movement. It is often familial, meaning it can happen in families, for example if one parent has a tongue tie, their baby could potentially have one too.
There are several types of tongue ties…
Generally the Hazelbaker classification (below) is widely used to describe the types of tongue tie that is present.
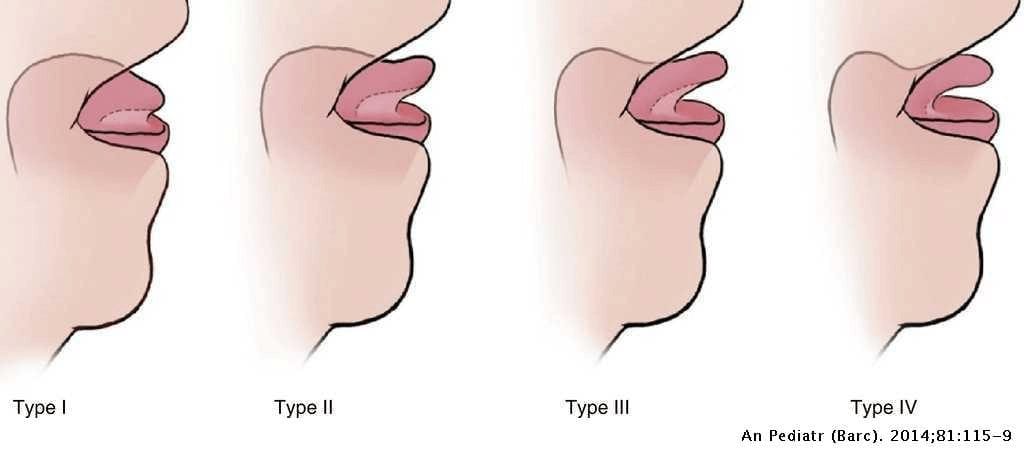
• Type I: thin and elastic frenulum; attaches the tip of the tongue to the alveolar ridge, and the tongue forms a heart shape.
• Type II: thin and elastic frenulum; 2–4mm behind the tongue tip, attaches by the alveolar ridge.
• Type III: thick, fibrous, and non-elastic frenulum; attaches mid-tongue to the floor of the mouth.
• Type IV: the frenulum is not seen, but felt, with fibrous or submucosal thick and shiny attachment from the base of the tongue to the floor of the mouth.
However, for a simpler and more functional assessment of the tied tongue, something like the Tabby assessment tool can be used to assess your child.

What are the Symptoms of Tongue Tie?
Symptoms may appear at different stages in life.
Though the severe type 1 may be immediately obvious at birth and highly likely to cause breast feeding problems and all the other issues as your child gets older.
The other types of tongue ties 2 to 4 may not immediately be obvious and it’s difficult to confirm that they would certainly cause issues later on in life.
Here we will describe tongue tie and its implications with Breast Feeding issues, Speech issues, Dental issues and finally Airway issues.
Tongue Tie and Breast Feeding issues
For efficient breast feeding, the latching process involves the tongue protruding out and creating a “suction-seal” on the underside of the mum’s breast/nipple and pulling in the whole of the nipple into the mouth whilst the upper gum massages on the breast (not the nipple or areolar), where the milk is stored, hence, drawing in the milk (see diagram below).
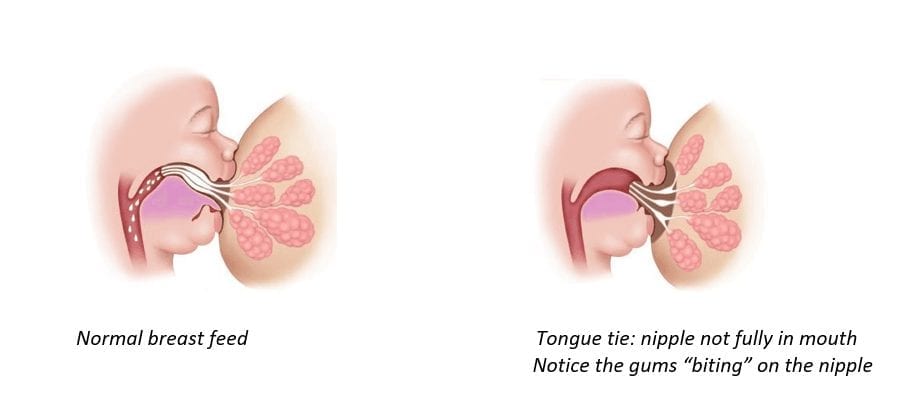
With a tongue tie, the tongue cannot protrude out enough and cannot form the suction seal adequately for good breast feeding to happen.
When the attempted suction comes off, this creates a clicky noise.
Symptoms of tongue tie causing breast feeding problems are:
- nipple trauma and pain for the mother,
- clicky noises when the tongue loose the seal on the breast,
- long duration or frequent feeding,
- drooling of milk during feeds,
- sucking and swallowing air thereby causing colic,
- dissatisfaction/ frustration after feeds requiring top up feeds,
- dehydration or prolonged jaundice,
- loss of interest to feed and weight loss.
Tongue Tie and Speech issues
Echoing the opinion of the College of Pediatrics, UK, not all tongue ties causes speech issues.
However speech problems will not be apparent until the age of 2 or 3 years old.
If a problem should arise, they may have difficulties with certain words such as, the “th”, “da”, “la” or “rrrr” sounds because their tongue cannot reach the roof of their mouths to form a seal. This may make them slur their words or sound unclear when they speak.
A speech therapist may be required to make an assessment and to do further work with their speech before and once the tongue tie is divided.
Tongue Tie and Dental Issues
One of the functions of the tongue is to clean the teeth after a meal.
It is usually an unconscious process and an inability to do this with a tight tongue tie, may allow food particles to get trapped between the teeth and predisposed your child to dental caries.
Another significant nonconscious function of the tongue is to govern the development of the facial skeleton and the upper jaw and teeth position.
With a low seated tongue (see diagram below), the upper teeth will be aligned more narrow and protruding forward causing a malocclusion on the sides and or overbite of the front teeth.

Tongue Tie and Airway Issues
The other significant potential problem that tongue ties could create is a high arched hard palate (roof of the mouth). This in turn makes the nasal air passages narrow.
Hence some kids may become chronic mouth breathers.
They may also have a possibility of having airway obstruction whilst sleeping. This may even present during childhood as snoring during sleep but also in adulthood with airway issues and obstructive sleep apnea.
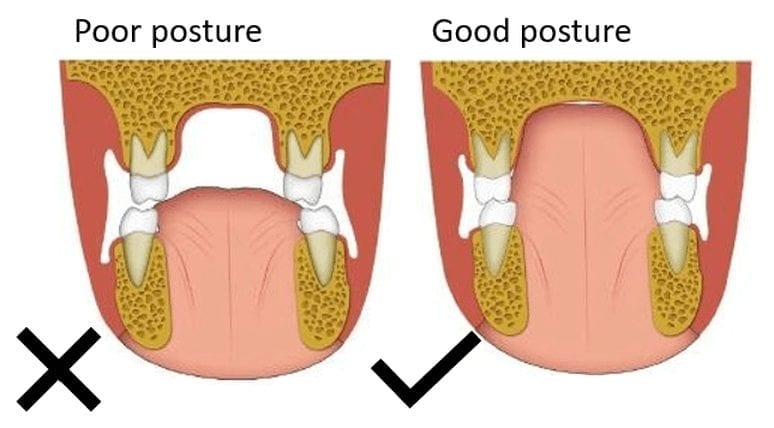
Left image above: The tongue tie creates a low tongue rest position and it creates a narrow upper teeth position with a high arch of the palate. It can create narrowing of the upper arch, chronic open mouth posture, and an unstable dental occlusion. This in turn creates a narrow nasal airway passage.
These children tend to be mouth breathers. They have a tendency of having their mouth open all the time and may even snore as a child, which is an abnormal sign.
Right image above: A normal tongue occupying the upper portion of the mouth and in contact with the palate. This encourages the more wide spaced upper teeth.
What is the Treatment for Tongue Tie?
Frenulotomy is the term used to cut the tongue tie.
In the first few months of life, this procedure can be done safely on the ward when the baby is first born or in the outpatient clinic.
Sucrose drops are given to the baby orally to reduce the sensation of pain. Once the baby is well swaddled , my assistant usually holds baby’s head with the mouth open. A tongue retractor is used to lift the tongue and the safe position of the tongue tie is cut, right to the angle of the tongue and floor of the mouth to free the tongue completely.
In expert hands, this process literally takes 3 seconds and that’s the duration of pain for baby, after this there should be no further pain.
A little pressure, using a gauze is applied to the cut area to slow down the bleeding from tiny vessels and soon baby will be placed on mum to directly breast feed.
You would feel an instant improvement in the way your baby feed and the pain for you should be much less or none at all. You will notice a diamond shaped raw surface under your baby’s tongue which will heal very quickly (see picture below).

The most important care required is to encourage your child to move his or her tongue which will stop it from joining back.
I usually teach parents how to do this after the successful division.
The best timing for tongue tie release would be within the first few weeks of your child’s life.
Dividing the tongue tie at this age is a very quick procedure with minimal risks and would certainly avoid general anaesthesia. You can then enjoy your baby feeding well from the start and not worry about any of the serious effects of tongue tie on to your child’s in later life.
The benefits of doing this far outweighs the small risk of the procedure. The earlier it is done, the better is for both mum and baby.
For children over the age of 1, they will usually require general anesthesia to have the procedure performed.
The vast majority of kids who had “missed” their tongue tie release as a baby will present to me at the ages of 2 to 3 years old with speech issues.
The procedure under general anesthesia will involve gaseous anesthesia in the operating theatre and once asleep, I use a bipolar instrument to seal and cut the membrane.
Once this is done a few stitches are applied to close the diamond shaped raw area to hasten the recovery and reduce the risks of the tissues joining.
Afterwards, they are taught tongue exercises to do at home and is back to normal almost instantly.

She had never been able to stick her tongue out of her mouth and the first thing she asked for is an ice cream to lick.
Prognosis (outcomes) of Tongue Tie Treatment
The main risks of tongue tie release are bleeding and recurrence (joining back). The risks however are very small. (extremely rare to bleed following breast feed and risk for re-joining is about 1 in 1500).
Most mother baby pairs do extremely well and often bonds much better too. With better breast feeding technique, breast milk production will also improve.
In our study in 2009 (see below) on the symptom which we could use to best predict a good outcome after tongue tie release, nipple pain and trauma for mother had the most likely mother-baby pairs to show maximum immediate improvement.

The recovery following the release under anesthesia is also very swift.
Children with speech issues are encouraged to follow up with their speech therapist to unlearn their previous way of tongue movement and learn the correct ways.
Something that I hear some parents of children who have the tongue tie snipped later is:
“I wish I had this done earlier or when he or she was a baby”















































